Lumbar disc prolapse: Symptoms and treatment
Following on from our blog on disc bulges, this week’s blog covers more specifically Lumbar disc prolapses!
It’s moving day and you’ve been running around packing, unpacking, lifting boxes and awkward furniture all day. You can’t stop though because there’s still more to do. It’s onwards and upwards with another load in the back of the Ute. You bend down to pick up the umpteenth box of the day and bang and you’re hit with excruciating low back pain and a shooting pain down the back of your leg. It’s crippling and you’re struggling to catch your breath and stand up straight.
It’s a scenario unfortunately a lot of us are familiar with, but what has caused this searing pain? One possible and relatively common cause for such pain is a lumbar disc prolapse. Let us take you through the ins and outs.
What is a disc?
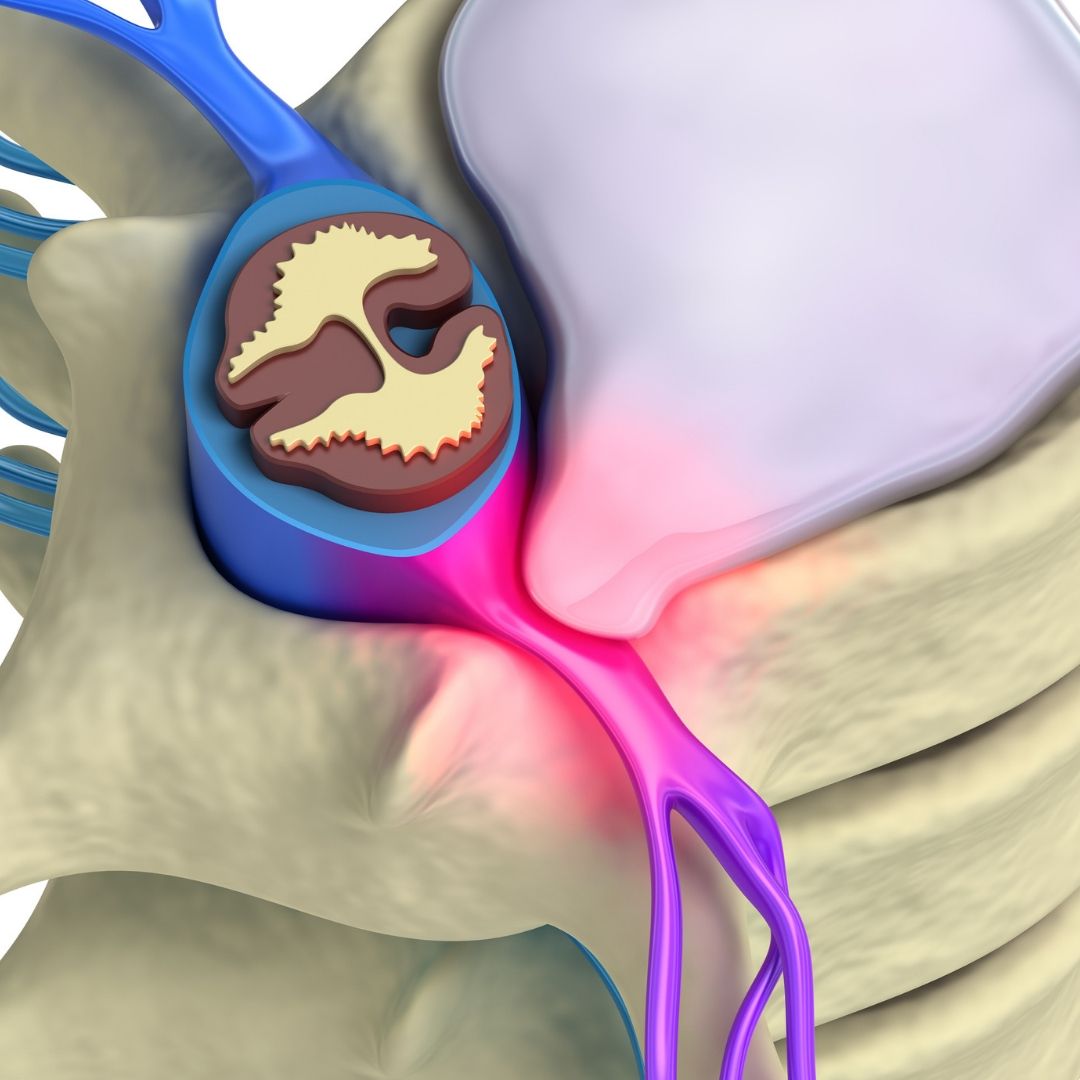
Your spine is made up of many vertebrae spanning from the neck all the way down to the tailbone. Between each vertebra sits an elastic-like structure called a disc. The disc is made up of a tough outer section called the ‘annulus fibrosus’, and a gel-like inner section called the ‘nucleus pulposus’. The discs work to separate the vertebrae to allow movement, as well as provide shock absorption to forces acting on the spine during movement.
What just happened when I bent down?
Common causes of disc prolapse include trauma and degeneration of the disc tissue as a result of poor posture (for example lots of slouching or slumping) and repetitive bending movements. When we bend forward, the forces acting on the discs, and especially the inner nucleus, increase drastically. Particularly when we bend forward under load, like with our house mover above who had been repetitively picking up and putting down heavy boxes.
Over time these repetitive movements may cause small micro-tears in the layers of the outer annulus, which weakens the overall structure of the disc. Slowly, the nucleus gets forced out and a small bulge may occur (there is often no pain at all at this stage). If these movements continue, or if you go to pick up that box which is just too heavy for you, the force is too much and the bulge can progress into a larger protrusion.
Like with any injury, the initial response of the body is inflammation. The presence of inflammatory chemicals alone can cause irritation to the surrounding nerve tissue as it exits the spine, or you may get actual contact of the disc on to the nerve itself, causing impingement. This is when you feel pain and know that all is not well.
What should I expect to feel when this happens?
The signs and symptoms of a disc prolapse can vary greatly depending on the type and severity of the prolapse, and where the spine is affected. A prolapse may happen slightly out to one side of the disc affecting only the nerves on that side of the body (this is most common). Or it may occur in a backwards direction, potentially affecting nerves on both sides of the body. A small bulge may only yield mild symptoms, whereas a large prolapse may cause more severe symptoms. Interestingly, this is not always the case though.
Some of the symptoms of a disc prolapse that you may experience include:
- Low back pain
- Pain running down the front, side or back of the leg
- Pins and needles or tingling down the leg
- Numbness down the leg
- Muscle weakness (this may manifest as losing the ability to lift your foot)
The most common disc prolapse affects the L5/S1 disc (the lowest disc in the spine) and will give symptoms down the side and back of the leg. Your practitioner will ask you lots of questions and do lots of tests to determine exactly what area is being affected.
How do we treat a disc prolapse initially?
Initially you may be in a lot of pain and simple movements may be very difficult to perform, like standing up straight, for example. This is because the body is trying to protect you from doing further damage. Once inflammation occurs, the body needs a few days to deal with what has happened.
So, if you come to see your Osteopath straight away, don’t expect to feel better after one visit. In fact, it is quite possible you will feel worse in the coming days before you start to feel better. The advantage of seeing your Osteo early on is that they can educate you on the do’s and don’ts, tell you what to look out for and inform you what to expect going forward. Often the unknown is scary, but your Osteopath will be able to ease your mind, even if not the pain immediately.
Us Osteopath’s like inflammation. It’s the body’s way of protecting the injury and getting organised for repair. So, although it may be painful, it is good to see it through without intervening too much.
What’s next?
Early on, we’ll get you moving better. We will also give you breathing, relaxation and core activation exercises to help the body better cope with the pain. A disc will often prolapse because of poor core stability, so getting you on the path to rehabilitating your core is good early on.
When it is possible, we will relax the tight muscles and reinstate movement to joints that may have seized up and become restricted following the injury. Our focus is to ensure the fluids of the body (i.e. blood, joint fluid, and lymphatic fluid) are moving freely around the body. When injury occurs, these fluids can become congested and a bit stuck around the area, and sometimes need a little help to get moving again. This will ensure a speedier recovery. The injury site will need lots of fresh blood to the area, while the lymphatic system will need to be flushed – ridding the area of all the bad stuff. Depending on the severity, discs generally take around 3-6 months to fully recover.
Your Osteopath is trained to help you through the injury process, so you can rest assured you are in safe hands. We know when and how to treat and know what to look for to ensure you are seen by the right people if it’s required (this might include your GP or a specialist if necessary).
If you think you have a disc prolapse or have previously been diagnosed with one and need help managing it, then look no further.
Call us today or book online to make your appointment.
References:
- Brukner, P. et al. 2017. Clinical Sports Medicine. 5th ed. Australia: McGraw-Hill Education
- Kim, Y. et al. 2018. Differences in the Incidence of Symptomatic Cervical and Lumbar Disc Herniation According to Age, Sex and National Health Insurance Eligibility: A Pilot Study on the Disease’s Association with Work. International Journal of Environmental Research and Public Health. 15 (10) 2094.
- Reiman, M. et al. 2016. Return to sport after open and microdiscectomy surgery versus conservative treatment for lumbar disc herniation: a systematic review with meta- analysis. British Medical Journal of Sports Medicine. 50. 221-230.